

Is Mitral Valve Repair Open Heart Surgery?
This page contains the following sections:
When is surgical repair of a mitral valve advisable?
How is repair of a mitral valve accomplished?
What are the risks and benefits of such surgery?
What is involved in a typical recovery?
When is surgical repair of a mitral valve advisable?
Image
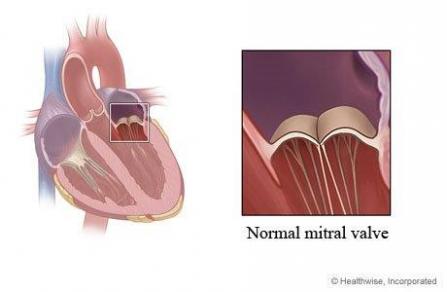
Your mitral valve is 2 lilliputian flaps of tissue that control the flow of blood from the upper chamber to the lower chamber on your centre'south left side. If it'due south seriously damaged, peculiarly if it'southward leaky, it is strongly advisable to consider surgical repair.
If you are diagnosed with a damaged mitral valve, your surgeon will evaluate the specifics of your situation—especially whether your valve is leaky (regurgitant) or blocked (stenotic). Then information technology will be possible to weigh the risks of surgery confronting the risks of managing the disorder with medication and other nonsurgical treatments. Sometimes, if your symptoms are not serious, they can be managed with lifestyle changes and/or medication. But often it will be appropriate, especially for a leaky valve, to consider surgery to accost the deficiency.
If your valve is severely leaky—as long as it hasn't been damaged by rheumatic fever and hasn't become calcified, or hardened—it is usually a good thought to repair the valve earlier information technology either results in significant damage to your centre or becomes so lacking that information technology can't be repaired and must exist replaced.
It is preferable to repair rather than replace a mitral valve, because a repaired valve by and large results in better heart function, better resistance to infection, and better long- and short-term survival. Studies have shown that patients who take a leaky mitral valve repaired before their heart function deteriorates render to a long-term survival curve the same every bit that of a general age-matched population. So with mitral valve disorders, it is important to give conscientious consideration to surgery before symptoms of congestive heart failure brainstorm to occur.
Should you and your surgeon decide the fourth dimension is right for surgery, go along in mind that mitral valve repair is a particular specialty of our cardiac surgeons. They take considerable expertise in all the proven options for repairing damaged mitral valves and a record of being able to repair nearly all leaky mitral valves not damaged by rheumatic fever and not calcified. We commonly perform surgical repair of the mitral valve.
How is repair of a mitral valve accomplished?
There are several ways to repair a damaged mitral valve. If your valve is judged to be repairable, the three primary matters your surgeon will consider are whether one or both of the tissue flaps that brand upward your mitral valve need repair, what kind of repair is most appropriate, and which surgical approach will work best.
Sometimes only ane of the 2 tissue flaps that make up your mitral valve needs repair, simply sometimes both practice. The flaps are as well known as cusps or leaflets; the mitral valve has a posterior leaflet (a C-shaped strip toward the back of your heart) and an anterior leaflet (a semicircle that fits into the open up side of the C, toward the forepart of your heart). The valve'southward proper name comes from the fact that the shape of the flaps looks somewhat like a miter, the formalism headdress worn past a bishop. (The mitral valve is also sometimes referred to equally the bicuspid valve—because it has two cusps, or leaflets. This can crusade confusion, however, because there is a mutual congenital defect, present from nascency, called bicuspid aortic valve; this is considering the aortic valve is supposed to have iii cusps, and then a bicuspid aortic valve is one with merely two rather than the normal iii flaps.) Our cardiac surgeons have considerable experience in repairing one or both flaps:
- Single leaflet repair involves repairing just the posterior leaflet or only the anterior leaflet. Some surgeons elsewhere take experience repairing only posterior leaflets.
- Bileaflet repair involves repairing both leaflets at the same time. Some surgeons elsewhere are not experienced in bileaflet repair.
There are 3 primary ways of performing the actual repair of a damaged mitral valve; these procedures are sometimes performed separately but are often used in combination:
- Annuloplasty involves repairing the ring of tissue to which the flaps are attached (this ring is known equally the annulus), by attaching a ring of tissue, cloth or metal to it.
- Resection involves trimming and/or reshaping the flaps themselves.
- Chordal replacement involves replacing one or more broken chords—tendons, as well known equally "centre strings," that attach the mitral valve's leaflets to the center—with Teflon.
The advisable surgical approach will depend on such factors every bit how damaged your valve is and the overall state of your health. Though open-heart surgery is the most common choice for mitral valve repairs, your surgeon volition decide which of the following procedures is nearly appropriate in your detail situation:
- Open-heart surgery to repair a lacking mitral valve involves making a 7- to 9-inch incision over the middle of the sternum, or breastbone, and so dividing the sternum to allow admission to the heart. In some cases a less invasive pick, involving a slightly smaller sternal incision, is possible. Then the damaged valve is repaired. It will be necessary to stop your heart from beating during the procedure, then the operation can be performed on a motionless and anemic field; while your center is stopped, a device known as a centre-lung bypass machine will accept over your centre's function and maintain your circulation.
- Minimally invasive surgery involves making 1 or two much smaller incisions (typically ii to 4 inches) in the side of your chest, between your ribs. And then the procedure is performed by inserting a tiny camera and long, thin surgical instruments through your tissues to your mitral valve. Minimally invasive surgery also requires the employ of a heart-lung bypass machine. Although it is typically not the preferable option for mitral valve repairs, in circumstances when it is advisable this approach avoids the demand to split the sternum and open the entire chest, so recovery may be faster.
What are the risks and benefits of such surgery?
It is of import to keep in listen that every medical choice involves a trade-off between risks and benefits—whether information technology is to undergo surgery, take medication, or even only carefully monitor a condition (an choice known as "watchful waiting").
In the case of a damaged or lacking mitral valve, deciding whether surgery is advisable involves balancing the risks involved in any heart surgery against the risk that managing the disorder with medication and other nonsurgical treatments may result in progressive damage to your heart and circulatory organisation or may crusade your valve to become so lacking that it tin can't exist repaired and must exist replaced. Studies accept shown that patients who don't have surgery to prepare a severely leaky mitral valve—even those who haven't nevertheless begun to bear witness symptoms—tin can suffer serious consequences; within x years, well-nigh ninety% will experience serious agin effects (such as congestive heart failure, an abnormal heart rhythm, or a stroke), and some will die.
By comparison, the risks involved in mitral valve repair surgery are extremely depression. A given patient's hazard volition vary, depending on such factors as historic period and overall wellness status, just the average mortality, or risk of death, from repair of a leaky (regurgitant) mitral valve is less than i%. Such surgery is also associated with a 1% risk of a blood jell that causes a serious stroke. In add-on, about i% of patients may later require an artificial pacemaker. And any surgical procedure involves a very small risk of other complications, such as infection.
Patients who fume can reduce their risk of complications if they end smoking at least two to 4 weeks before their surgery (it is best not to quit immediately before having heart surgery, however, because when people stop smoking they often have short-term bronchorrhea, or backlog secretions in their respiratory tract, which makes them coughing a lot—and cough a lot when you have only had heart surgery is non a good idea).
The benefits of successful surgery are considerable. The overwhelming bulk of patients, one time they recover, feel better than they did before the operation and are able to resume any activities they wish to engage in. Repairing a mitral valve usually not simply fixes the damaged valve but besides relieves all the patient'due south symptoms, results in improved brusk- and long-term survival, and in many circumstances returns the patient to a long-term survival curve the aforementioned every bit that of a full general age-matched population. In add-on, many patients whose mitral valve is successfully repaired are able to stop taking take claret-thinning medication (oftentimes referred to past the make name of Coumadin).
What is involved in a typical recovery?
A typical open-heart process takes from 4 to 6 hours, in some cases up to eight hours; patients are then maintained under general anesthesia for an additional 4 to 6 hours. If their middle is performing well and there is no backlog bleeding, they tin emerge from anesthesia and have their breathing tube removed. About patients stay in the ICU until midday of the day after their procedure; if they continue to do well, the drainage tubes in their breast tin can then be removed and they tin can exist moved to a regular hospital bed later that day.
The typical hospital stay ranges from four to vii days. At that point, the vast bulk of patients are able to go home, with support from the visiting nurse service, though about 15% to 20% may need to spend some time in a rehab facility for more extensive rehabilitation. After discharge, patients are advised not to bulldoze for nigh iii weeks and non to elevator anything heavier than 5 pounds for about half-dozen weeks. Beyond that point, they can resume whatever activities they wish to.
Patients tend to exist surprised at how piece of cake it is to control their pain. By the second day after their operation, most patients are comfortable without intravenous hurting medication, taking only oral painkillers, and the overwhelming majority are discharged home on simply Tylenol or Motrin.
In cases when minimally invasive surgery is appropriate, both the length of the operation and the recovery catamenia are typically shorter.
Page reviewed on: Jun 26, 2022
Folio reviewed by: Jock McCullough, Physician

Source: https://www.dartmouth-hitchcock.org/heart-vascular/mitral-valve-repair
Posted by: brockpoliose.blogspot.com
0 Response to "Is Mitral Valve Repair Open Heart Surgery?"
Post a Comment